
Written by Tracy Coval for the RSDSA blog.
Tracy Coval gives RSDSA a look into her life with CRPS and dystonia. See what she has done through her journey. Note this was initially posted on her blog, which can be found at this link (click here). Some of the images may be too graphic for some readers.
I was first diagnosed in 2002 with Complex Regional Pain Syndrome (CRPS/RSD) when I was 11 years old after a running injury. I was running in gym class and twisted my left ankle in. When I told the gym teacher I couldn’t run anymore, he wouldn’t believe me and had me keep going. The pain kept progressing, and I saw an orthopedist who diagnosed me with Tendonitis and put me in an air cast. The pain continued, and my ankle/foot was turning purple. After going back to the orthopedist 2 more times, the doctor finally told my mom, “I’m sorry but this is all in your daughter’s head. You need to get her psychological help”. After getting in an appointment with an orthopedic surgeon at Boston Children’s Hospital, I would learn of the name Reflex Sympathetic Dystrophy (the name was changed a year or so after to Complex Regional Pain Syndrome).
CRPS/RSD is a neurological disorder that causes pain waves to be sent to the brain, telling the brain that you are in chronic pain, even though nothing is wrong. CRPS/RSD usually develops after an injury, surgery, or even something as simple as a blood draw. CRPS/RSD is known as the ‘suicide disease’ as many people can’t handle the pain anymore. The disease is rated on the McGill pain scale as being more painful than amputation, or giving birth naturally. CRPS usually develops in a limb, but there are cases where individuals are affected by it throughout their entire body. This is known as full body CRPS. The pain is the worst pain one could encounter. The pain feels like you are lit on fire, on top of stabbing, throbbing and aching pain. Think of sticking your hands in a bucket of freezing cold ice water and not being able to take your hands out of it. No one really understands CRPS, but the sooner you are diagnosed, the better chance you have to go into remission.
I would be told that I would need to be referred to a pain clinic, and that this would resolve on it’s own. Boy was this doctor wrong. I would learn that I would have CRPS for the rest of my life. A common phrase that was heard by my main provider was, “suck it up and live”. I was 11 when I heard this for the first time. I would then try every medication, nerve blocks, epidurals, lidocaine infusions, acupuncture, reiki, herbal remedies and more with no relief.
At the age of 14, I was sent to Children’s Hospital of Philadelphia (CHOP) to attend an aggressive physical therapy program. The goal was to retrain my brain to understand that non painful stimuli would not make my pain worse. This is known as desensitization and it’s done through physical activity. Treatment was scheduled Monday through Friday, 7 hours a day. The staff were comprised of physical therapists, occupational therapists, social workers, art therapists, music therapists, and the main doctor.
The doctor running this programed believed it was crucial to be taken off all of your medication, and treated CRPS more as a psychological issue than a neurological issue. Both the physical therapists and the occupational therapists reminded me of drill sergeants; their approach towards the exercises were aggressive. In PT, I was pushed to my limits with many exercises, especially the ones where I was required to beat my record of the amount of reps I could complete in a minute. If I didn’t do more than my previous record, I would have to do it again. There were many tears, and too many vomit buckets to count.
After being there for two weeks, I had a few falls to my left arm, and I remember feeling this stabbing burning pain. It was discolored and swollen, and I couldn’t touch it. X-rays were performed and it was determined that the RSD had spread.
After being at CHOP for 1 month, I was finally discharged after being there for 1 month. The pain in my left ankle/foot and knee was gone but my left arm was horrible.
The pain relief in my left leg lasted for a year, and it was amazing. I went back to dancing 5 days a week, while doing physical therapy on my left arm. There was one day I was in dance, and I felt that familiar pain that I hoped would never come back. I followed up with my doctor at Boston Children’s who said there was nothing more that he could do for me.
At this time, I was finishing my freshman year of high school. I would now be on my own handling the pain. My mind set was to ignore the pain, and continue to do the things that I loved: art, dance, and cheerleading. By junior year of high school, I had taken a break from dance, as I fractured my spine. This recovery lasted for a year and a half. After getting cleared to return to activities, the CRPS was intensifying. I was noticing I was going through frequent flares, missing a lot of school, and it was getting harder to walk. I am amazed and proud to say I graduated high school.
2009 I started college at Lesley University in Cambridge, MA. I was excited to finally have the college experience. I was continuing dance and cheerleading, but realized I really needed help with the CRPS pain. After talking with a family friend, I got the name of a pain doctor who I still use to this day. The best part is he looks like Kramer from Seinfeld. I was his youngest patient at the age of 19. His treatment plan was to do a Spinal Cord Stimulator (SCS). A SCS is a mild electric current to your spinal cord. The goal is to block out the pain receptors by feeling the electric current instead. I went through the trial run, and found it extremely helpful. The trial gave me hope that I could go back to dance. I had my first SCS implanted December of 2011, my junior year of college. I had it done during my winter break. The SCS is a 6 month recovery that requires you not to bend. The pain from the surgery was extremely painful, but my CRPS pain was getting more tolerable, and I found I was finally getting relief. I am so grateful for all of my friends in school who were so helpful and understanding. My friends were awesome for pitching in, and I was fortunate that my professors were understanding of the surgery. After 6 months, I was back to dancing with my team. Words can’t explain how it feels to go back to something that you loved so much that had been taken away from you for so long. I was so happy, and really felt I was getting my life back. I was doing an art therapy internship with a pediatric inpatient psychiatric unit for over a year, and I was interested pursuing a career in social work.
After dancing for a year, I began feeling pain in my right foot. My foot was becoming discolored and was ice cold to the touch. When I followed up with my pain doctor, he confirmed the CRPS had now spread. He felt it was time to try a medication called Ketamine. Ketamine is mainly used during anesthesia, but there is reports that it helps treat CRPS. I would start with ketamine lozenges (it looks like the size of a starburst), and then I would go for infusions. The infusions would take 4-6 hours, and often I would be extremely out of it because of the side effects.
It was exciting to see how much the Ketamine was helping. I wasn’t missing as many classes, my flares were not as severe, and I was finally enjoying college more because the pain was better. I would go for infusions every 8 weeks, while being in my senior year of college. By my second semester, I started working on an inpatient psychiatric unit specializing in eating disorders, and ecstatic to learn I was accepted into my top choice for graduate schools. I graduated Lesley University with my Bachelors of Science May 2013
Fall 2013 I started graduate school, while continuing to work part time. I was really busy, but happy with everything I was learning. My pain was still there but it was manageable thanks to the Ketamine infusions. Unfortunately, my treatment approach was about to change, as my health insurance stopped covering the ketamine infusions, and the ketamine lozenges. My doctor fought the insurance providers for months, but they wouldn’t budge. Next treatment plan: another spinal cord stimulator for the right side of my body. When I had the first SCS implanted, it was designed to control one side of the body. A year after I had my SCS implanted, a newer model came out where there is now an ability to get full body coverage. My doctor felt it was best to keep in my first one, and put in a second device. It was decided I would have this surgery done after I finished finals, and recover during winter break.
Two months before my surgery, I started having some issues with my job. Because the ketamine infusions had stopped, my flares were getting worse, and there were shifts I had to call out on. I had met with my nurse manager and had explained about CRPS, and had asked her if she wanted documentation. Her response was no. After a couple of weeks had gone by, I was called in to meet with the Director of Nursing who scolded me for calling out because she thought I was out partying and lazy. (I wish I was joking about this). I started hysterically crying and trying to explain I had a neurological disorder, and made sure to explain that my nurse manager was aware. I explained I was going to be needing neurosurgery again and it is out of my control when the pain flares occur. She asked to get the documentation, and set up a time to meet with human resources to talk to them about this. Once I met with human resources, I learned that my job would not be held when I come back from surgery, and I was let go from my position.
I had the surgery December 2013, and it was a rough and painful recovery. I would go to classes sitting on pillows, in attempt to try and be semi comfortable. I knew I needed to continue school as a distraction from the pain. Once I got through my 6 month recovery, my friend helped me get a job working at an emergency room working as a Patient Safety Assistant. Often, I would be working with psychiatric patients who were on a section 12, and needed supervision for safety reason.
Fall of 2014 I started my second year at school, and was assigned my first field placement; a homeless shelter for children in state custody. I was having difficulty balancing work, an internship, school, and RSD. I was offered at my internship an opportunity to be paid to work as a social worker on top of doing my school internship. For me this felt like the right fit as my internship was a shorter commute than my job at the ER.
Summer 2015 I decided I needed to take care of myself, and my whole self. I have struggled with weight all of my life, and had tried many different approaches to lose weight, and I was never successful. I decided to meet with a bariatric specialist, and after a lot of consideration and research, I decided to get the lap band. The lap-band is an adjustable silicone band placed around the top part of the stomach, designed to restrict food intake. At the time of surgery, a small device called a port (or reservoir) is placed under the skin of the abdomen. I wanted to lose weight on my own, but I knew that I needed help. Weight loss surgery is NOT a quick fix to losing weight; it is a tool to help. Weight loss surgery is a complete life change, and I was ready to take on that change. I had the surgery done on August 11, 2015 and I went into surgery smiling because I knew this was going to help my overall health, but especially the RSD. To this date, I have lost 100+ pounds, and I have never been so proud. It was worth the change, and I did not realize how important your diet is especially with a chronic illness.
I entered my last year of school, Fall of 2015, and my next placement was at a homeless shelter for pregnant teen and teen moms. I had been having a lot of muscle spasms, especially in my feet. My toes would curl and get stuck at times from the muscle spasms cramping my toes. I thought this was from the RSD and really didn’t think much of it. When I would bring this up to my pain doctor, he wasn’t sure why the cramping was so severe. I remember laying down on the couch Saturday morning with the worst muscle spasms. I took my meds hoping it would help loosen them. 2 hours later the muscles spasms were continuing and were so severe I was hunched over crying from the pain. My toes were curled and I was having uncontrollable cramping. It felt like the worst Charlie horse that would not release. 911 was called as I couldn’t move. My legs were locked, and it was the most frightening moment of my life. Paramedics had to carry me out of the house as I was howling from the contractions. After being in the ER for 6 hours, I was discharged, and told to go see my pain doctor immediately. I got an appointment with him a week later and described to him the symptoms and the ER event. I would learn I have a condition called Dystonia, and he informed me that he doesn’t treat this. He warned me that if this happens again, where I get locked in contractions, then I have to go to the ER ASAP to break the abnormal posture before my brain thinks this is the way my toes should be positioned.
Dystonia is a movement disorder where you have uncontrollable muscle contractions. Usually body parts will twist involuntarily, have repetitive movements and/or can often get stuck in different postures. I would later learn that often times CRPS/RSD and Dystonia like to be best friends. Not always, but it can happen.
After my first initial diagnosis, I would be in the ER two more times due to my legs locking up, one of the situations happened while I was driving and lost control of my car. I was hospitalized for 9 days, and all of the doctors felt that this was psychological and I was a drug seeker, even though my toes were stuck in a curled position. I was sent to a rehabilitation center for another two months. All of the doctors there tried different medications, Botox, physical therapy, and occupational therapy and nothing was getting better. The doctors all had team meeting and felt it was time I be transferred to another hospital as they felt that I need further help with pain control, but they also felt this was mainly psychological. I was transferred to another hospital to have a psychiatric evaluation performed per request by the insurance company. The three doctors who were in charge of my case felt this was not psychological, and felt it was in the best interest to be transferred to a Boston hospital to work with a Dystonia clinic. I was in the hospital for three days, and then finally discharged and wheelchair bound.
During the next couple of months, I would be tossed from specialist to specialist all agreeing that my case was too complicated, and there was nothing they could do. One doctor referred me to a neuropsychiatrist at Massachusetts General Hospital, and my appointment wouldn’t be for another 6 months. During this time, I taught myself how to walk again using forearm crutches. I did not have any form of physical therapy during this period, so I forced myself to practice every day, several times a day. I took myself off all of the opioids, muscle relaxers, and benzodiazepines. I decided to use medical marijuana to help with the pain and muscle contractions, which was one of the best decisions I have made. I was tired of having so much medication, and I wanted to prove to the doctors I was not faking this.
When I finally had my appointment with the neuropsychiatrist, I was amazed he spent an hour and a half with my dad and I. He agreed this was a form of Dystonia, and this was not psychological. I would then be referred to a neurologist who specializes in Dystonia. This specialist would spend over 3 hours with me for my first appointment. Apparently, there are several types of Dystonia’, but often physicians are not educated about Functional Dystonia because the United States is not up to date when it comes to Functional Neurological Disorders. Apparently, the United Kingdom is extremely educated on this, and if I was in the UK, the muscle contractions could have been reversed because there is a proper treatment team protocol that is used when a patient starts to show signs of a Functional Dystonia. The sooner it is caught, the faster it can be treated. I had learned during this appointment that if I got to this neurologist soon enough, this all could have been reversed. I would then be referred to a physiatrist to determine if my ankles/feet/toes could be saved.

While waiting to see the physiatrist, I would travel to Rhode Island to meet with Dr. Pradeep Chopra on May 24, 2016. Dr. Chopra is very well known for CRPS and his diagnostic work. After spending over 5 hours with my dad and I for our initial visit, another diagnosis added to my medical terminology list: Ehlers-Danlos Syndrome (EDS). EDS is a genetic disorder you are born with that affects your connective tissue. Usually this is seen with joint hyper-mobility, skin hyperextensibility (my skin is really stretchy, I know gross), and fragile tissue. Dr. Chopra was able to help me understand that I was born with EDS, and the EDS most likely caused the CRPS, and the CRPS caused the Dystonia. Dr. Chopra also felt something else was going on with my spine, but that will be discussed another day.
In September of 2016, I would meet with the physiatrist, who did a nerve block to numb my leg, and see if he could break the contractions. His thought was if my brain couldn’t feel the pain then the contractions would break; my toes never moved no matter how much he forced it. I learned that my toes were paralyzed, and my ankles were frozen. I was told it was time to meet with an orthopedic surgeon as I would need surgery. I was told it could be either reconstructive surgery, or amputation.
After waiting a month, I got an appointment with an orthopedic surgeon who is the Chief of Orthopedic Surgeons for Brigham and Woman’s Hospital. He looked at my feet, and said he didn’t even know if he could get to the tendons in my toes because of how severe the contractions were. He wanted to do a further exam by putting me under anesthesia and seeing if my toes would relax. We tried it with no such luck. The surgeon brought in 8 opinions to see what my best option was. All of the doctors felt amputation was most likely what was going to happen, but here was the action plan: tendons would be severed in each toe, bone would [be] removed from each toe, and pins would be placed. I was told to prepare for amputation as the surgeon was unsure that my skin would hold up when it came to suturing the wounds, and the plastic surgeon felt that I was not a good candidate for a skin graft. I learned this surgery will not fix the Dystonia, or my ankles, but it will help my walking and pain in the long run. Both feet have to be done, but the left foot will go first as it is the worst out of the two.
The first surgery was done on March 28, 2017 and I woke up with all of my toes. There were so many tears of joy and happiness as everyone is amazed this happened. I was given a 90% chance that I was going to wake up from surgery needing amputation on half of my foot. All of the doctors have been preparing me for amputation, so that was what we were all anticipating. I was under the knife for four and a half hours, as the surgeons worked as hard as they could. All the tendons of my toes were severed, bones were removed, and I also have a bone fusion for my big toe where the knuckle is.
On June 30, 2017, the second surgery was performed. During this procedure, the pins were removed from all of my toes, and my facia muscle was cut. The purpose of cutting the facia muscle was to see if it would lengthen the Achilles tendon. The surgeon and the Dystonia specialist explained that if we did not do work on my tendon, I would never be able to walk again.
My foot morning of surgery 3/28/17

My foot morning of surgery 3/28/17

The first time looking at my foot after surgery 3/28/17

2 weeks post-operative after the pins were taken out and the facia muscle was cut

Please consider making a donation to RSDSA today!
 Written by Ashley Epping
Written by Ashley Epping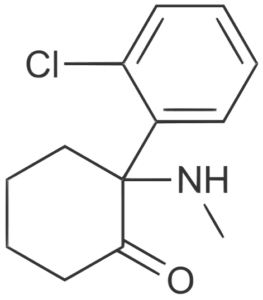 Written by Guest Blogger Allison Wells, MD
Written by Guest Blogger Allison Wells, MD Written by Guest Blogger Suzanne Stewart
Written by Guest Blogger Suzanne Stewart Written by Guest Blogger Melissa Lovitz. Melissa initially featured this post on her
Written by Guest Blogger Melissa Lovitz. Melissa initially featured this post on her  Written by Guest Blogger Victoria Abbott-Fleming
Written by Guest Blogger Victoria Abbott-Fleming Written by Nurse Beth Seickel for the RSDSA Blog
Written by Nurse Beth Seickel for the RSDSA Blog Written by Guest Blogger Stephanie Umlor for the RSDSA blog.
Written by Guest Blogger Stephanie Umlor for the RSDSA blog. Written by Guest Blogger Melissa Lanty
Written by Guest Blogger Melissa Lanty